Dr. Vladislav Zlatinov
Graduated as Master of Veterinary Medicine in 2005 in Sofia.
From 2005 to 2009 worked as a general practitioner at the Animo Small Animal Veterinary Clinic.
Since 2009 working as a chief veterinarian and senior surgeon at the Central Veterinary Clinic - Sofia, gaining main clinical experience and became a specialist in the field of orthopedics and spinal surgery.
In the last 5 years, the main focus of my work has been referred surgical cases, requiring complex diagnostic and therapeutic activities.
From 2021 started working as a freelance surgeon.
Memberships and recognitions
2012: co-founder of the Bulgarian Association of Veterinary Orthopedics and Traumatology (BAVOT). Currently President of the Organization.
2013: certified member of GRSK - FCI recognised organization for control of genetic diseases of the skeleton (internationally certified panelist for elbow and hip dysplasia).
2015: co-founder of Veterinary Orthopedic and Neurology Group (VOG) - Slovenia.
2015: AOVET - active member, speaker / instructor (AOvet faculty).
Practical trainings and certificates
2007: two-week externship in the surgical department of the Clinic Mediterraneo, Madrid, Spain, under the direction of Dr. Miguel Ruiz Fundador and Dr. Margot Ruiz - general orthopedic and neurosurgery cases.
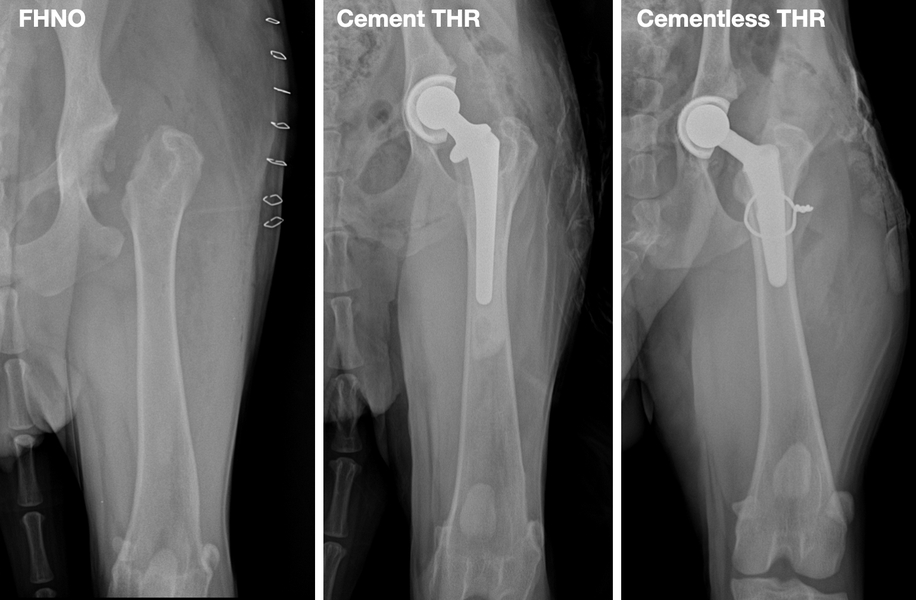
2012: course and certification program for Total hip replacement - BIOMEDTRIX Universal Hip - Bristol, UK.
2014: two-week internship at Clinica Parabiago, Milan, Italy, under the guidance of Dr. Luca Redelli. Training with emphasis on TPLO technique for ruptured cranial cruciate ligament and distraction osteogenesis (Ilizarov’s method).
2014 AOVET courses:
- Principles in a Fracture management; Zagreb, Croatia;
- Advances in Fracture management; Cremona, Italy;
- Master class on advanced corrective osteotomies: Rear limb and Patellar luxation, Cremona, Italy.
2014: one-week externship at the Faculty of Veterinary Medicine, Turin, Italy, under the guidance of Professor Bruno Peirone. Training with focus - traumatology, TPLO technique for ruptured cranial cruciate ligament.
2015: conducts 8 weeks AOvet fellowship internship at Clinica Veterinaria - Dr. Aldo Vezzoni, Cremona, Italy, with emphasis on diagnosis and treatment of hip and elbow dysplasia, total hip arthroplasty (Kyon THR), TPLO, arthroscopic diagnosis and treatment.
AOvet fellowship: a sponsored postgraduate program in orthopedics.
Speaker / instructor in regional seminars
Frequent speaker in national seminars - BAVOT and others.
Instructor of practical courses (wet lab) - X-ray examination of the skeleton, Surgery of the stifle joint, External skeletal fixator for the treatment of fractures held in Central Veterinary Clinic - Sofia.
“Osteosynthesis with plates” (dry lab), Mikromed sponsored seminar, Sofia.
TPLO technique for ruptured cranial cruciate ligament (International wet lab), VetWest, Sofia.
International speaker / instructor
“Advanced Orthopedic Workshop” - Opatija, Croatia, 2016.
“Juvenile orthopedic diseases”, VOG - Zagreb, Croatia, 2017.
“Sankt Petersburg International Vet Conference” (Russia), 2016 and 2017.
“CORA based TPLO”, practical course, St. Petersburg, 2017.
Fracture treatment principles, Limassol, Cyprus 2017.
Main speaker in the orthopedic section of the National Veterinary Conference - Moscow, Russia, 2018.
“Traumatology Seminar” - VOG, Zreče, Slovenia, 2018.
“Fracture treatment by plate osteosynthesis”, practical course, Bucharest, 2018.
Lecturer in the orthopedic section of CONGRESO INTERNACIONALVETERINARIO DE LEON- Leon, Mexico, 2019.
International lecturer / instructor Intrauma (Fixin) courses
“FIXIN wet lab on TPLO and DPO” - co-lecturer with Dr. Luca Vezzoni - practica lcourse, Opatija, Croatia, 2017.
“TPLO dry lab-basic course” - co-lecturer with Dr. Massimo Petazzoni, practical course, Bucharest, Romania, 2017.
Fixin international symposium - case presenter at round table discussion, Venice, 2017.
“Angular bone deformities - hind limb” - co-lecturer together with Dr. Luca Vezzoni, practical course, Opatija, Croatia, 2018.
“TPLO dry lab” - co-lecturer together with Dr. Luca Omodeo, practical course, Larnaca, Cyprus, 2019.
“Second Intrauma Symposium” - speaker, Turin, Italy 2019
AOVET faculty / table instructor
"Small Animal Master Class - Small and Toy Breed Dog" - Dubrovnik, 2016.
“Masters in Small Animal - Tibial Plateau Levelling Osteotomy (TPLO)” - Lisbon, Portugal 2017.
“Canine Sports Medicine Orthopedics and Traumatology”, master course, Dubrovnik, 2018.
“Avian and Exotics Orthopedics”, master course, Dubrovnik, 2018.
Asian Veterinary Orthopedic and Neurological Conference - Xian, China, 2019
Three days courses and lectures:
- Dynamic Ulna Osteotomies and Proximal Abducting Ulnar Osteotomy (PAUL), Patellar Groove Replacement (PGR) for Patellar Luxation
- AO VET Surgical Secrets
- Complex Cases and Advanced Surgery
Other
Co-organizer in the planning and conducting of over 10 seminars with international lecturers of the Bulgarian Association of Veterinary Orthopedics and Traumatology (BAVOT).
Author of 15 publications in regional scientific journals (including online publications) - articles and clinical reports.
One of the first veterinary surgeons to introduce in Bulgaria - total hip replacement, TPLO technique for ruptured cranial cruciate ligament, arthroscopic method for treatment of orthopedic diseases and others.
The first surgeon in Bulgaria to introduce transcutaneous integrated limb endoprosthesis (still a highly innovative technique worldwide).








 AO VET Dubrovnik, 2017
AO VET Dubrovnik, 2017  AO VET Lisbon, 2019
AO VET Lisbon, 2019  BAVOT, 2019, corrective osteotomy of the hindlimb
BAVOT, 2019, corrective osteotomy of the hindlimb  BAVOT, seminar with Mike Farrell and Ignacio Calvo, 2018
BAVOT, seminar with Mike Farrell and Ignacio Calvo, 2018  BAVOT, seminar with Prof. Bruno Peyrone
BAVOT, seminar with Prof. Bruno Peyrone  Intrauma symposium, 2019
Intrauma symposium, 2019  Leon Congress, Mexico, 2019
Leon Congress, Mexico, 2019  AO VET, Pan-Asian Conference, 2019
AO VET, Pan-Asian Conference, 2019  TPLO workshop with Massimo Petazzoni, 2017
TPLO workshop with Massimo Petazzoni, 2017  VOG seminar, Croatia, 2016
VOG seminar, Croatia, 2016 


















































{kind=link}
{kind=link}